
Here we discuss normal TSH levels and review data from several studies to learn about the ranges of thyroid hormones.
Thyroid hormones are extremely important for our health.
In fact, normal thyroid levels are necessary to avoid serious consequences to a child's growth and development.
Hypothyroidism and hyperthyroidism are two common disorders with abnormal TSH levels (thyroid-stimulating hormone is also called thyrotropin).
In general, the risk of thyroid disorders during our lifetime is quite high.
The risk increases with age and seniors are most affected.
Thyroid problems in women are more common: almost 1 in 7 women maybe at risk.
A study from Denmark suggests overall risk of overt (i.e., clinical stage) hypothyroidism or hyperthyroidism diagnosis, during a person's lifetime, is close to 10% (Carle’ 2006), as the graph below shows.
Women are four-times at higher risk than men.
For US, Europe, and other developed countries, where iodine deficiency is rare, the risk is comparable.
Regularly testing thyroid levels is one way to reduce this risk.
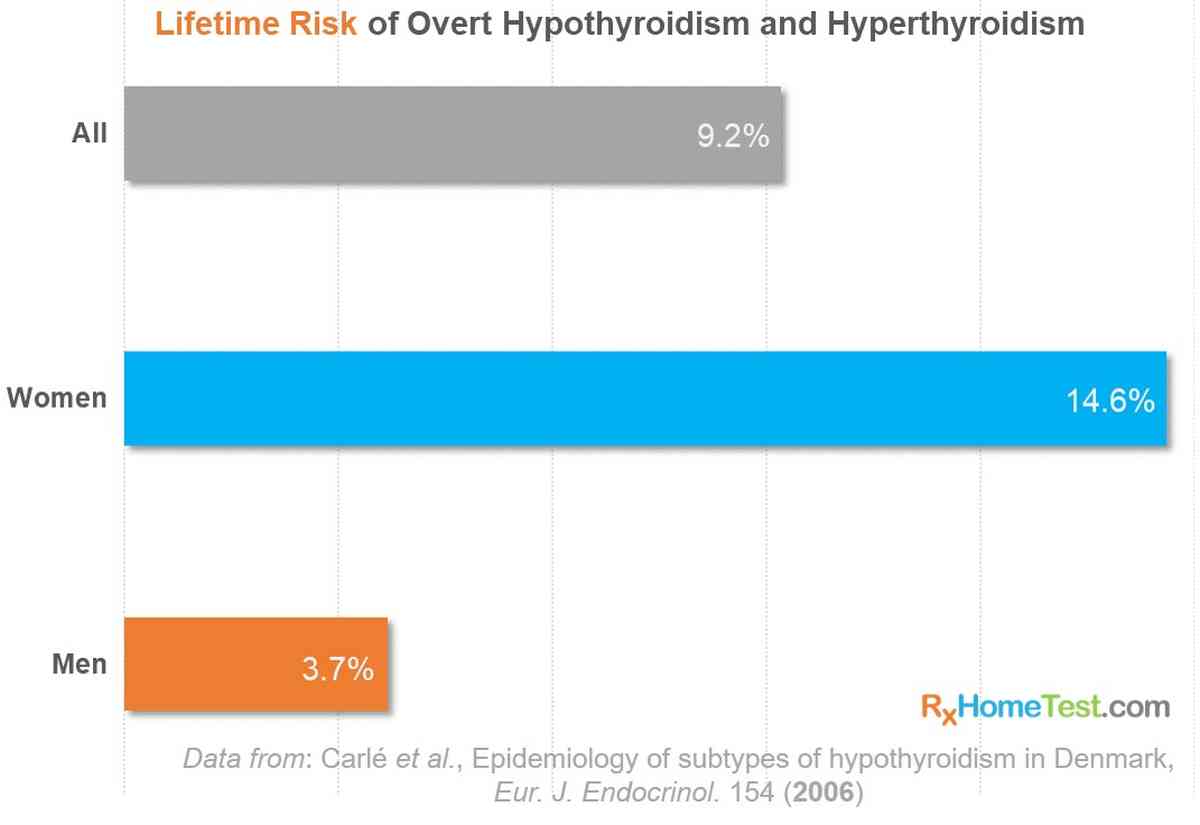
Chart showing the risk of thyroid problems during a life time
"Epidemiology of sub-types of hypothyroidism in Denmark" by Allan Carlé and others in European Journal of Endocrinology, vol. 154 (1), 2006.
Order an At-Home Thyroid Test.

Order an At-Home Thyroid Test.
MORE FROM OUR BLOGS:
Thyroid and Your Health – how thyroid impacts almost everyone.
Pregnancy and Role of Thyroid – why thyroid health is critical during pregnancy.
Learn All About Thyroid – summary of thyroid disorders and their symptoms.
Tips for Understanding Thyroid Test Results – ranges for TSH, free T4, free T3, and TPO.
The chart below shows ranges for normal TSH levels.
It also includes the lab ranges for other key thyroid hormones and TPO antibodies–a marker of immune response against the thyroid gland.
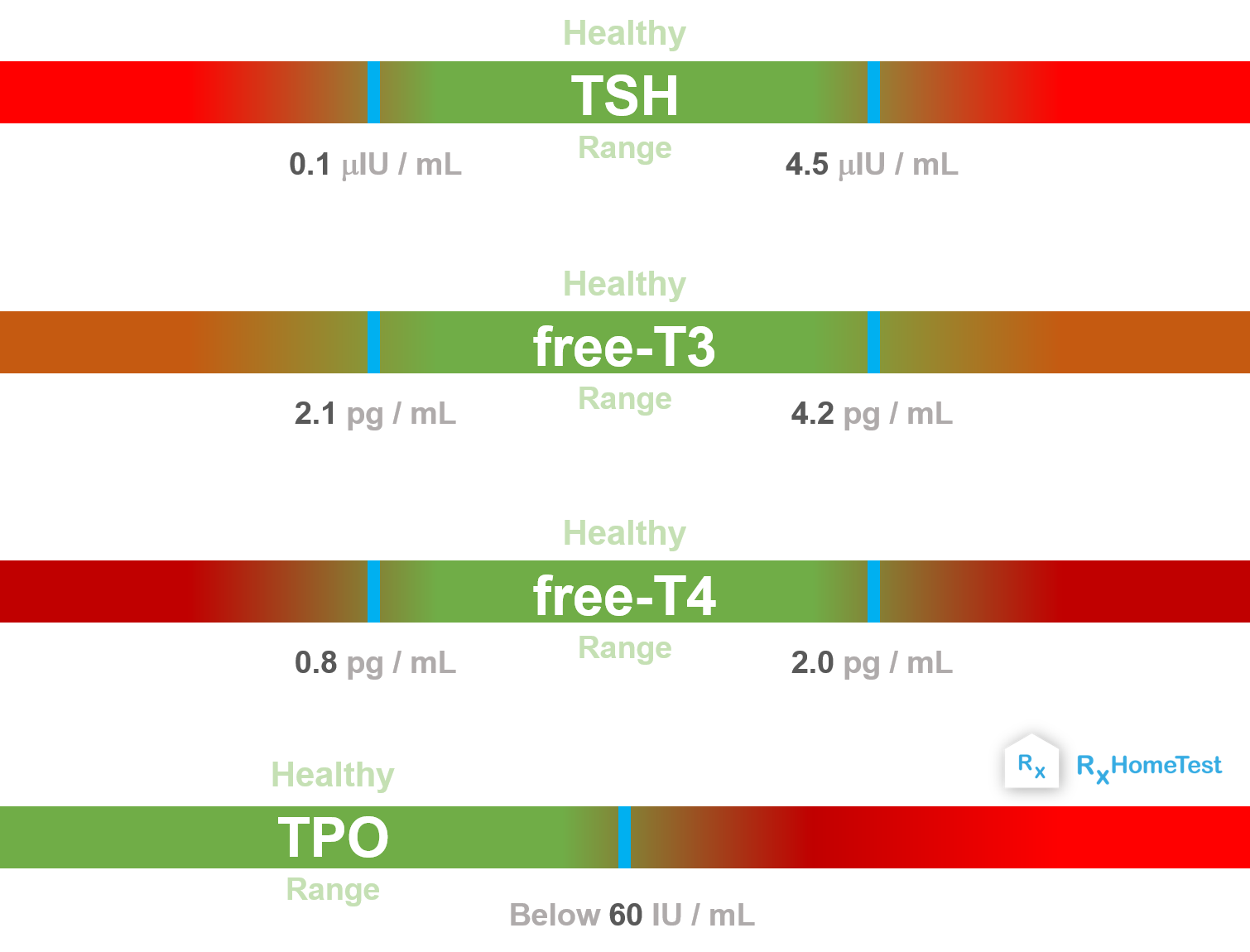
Chart showing normal range for TSH, free T3, free T4 and TPO antibody levels for one of our at-home thyroid tests.
The distribution of Thyroid Stimulating Hormone in healthy population is close to a bell curve (but it is asymmetric, i.e., non-Gaussian distribution).
The curve skews to the right—that means, high TSH levels seem to be more common than TSH low levels.
Optimal TSH levels range between 0.1 mIU/L and 4.5 mIU/L.
Statistically, that's between 2.5th and 97.5th percentile (±2 standard deviation).
This means 95% of the people have thyroid levels in this range.
Age, gender, race, and iodine consumption can cause variations.
The most common value of normal TSH levels is around 1.2 to 1.5 mIU/L (or µIU/mL), as seen from this plot below.
This plot below shows distribution of normal TSH levels in women from a Danish study around 2000 AD.

Chart showing range of TSH levels in a large study of 8,000 people from Denmark.
"Lower prevalence of mild hyperthyroidism related to a higher iodine intake in the population: prospective study of a mandatory iodization programme" by Vejbjerg & others, in Clinical Endocrinology, Vol 71 (3) 2009.
Problems with the hypothalamus, pituitary, or thyroid gland can cause affect normal TSH levels.
Here are few other common factors that play a role:
The 24-hour trend below shows Thyroid Stimulating Hormones vary in two different cyclical patterns (Weeke and Gundersen 1978). T3—and even T4 to a less extent—follows similar trend.
During the night while sleeping, TSH increases by almost 150% in comparison to day time. As we wake up, it decreases slowly. Therefore, results can vary appreciably depending on the time of sample collection. This trend over 24 hour is called diurnal or daily rhythm.
The pituitary gland in our brain releases this hormone in short pulses. The levels rise by about 10-15% every 30 minutes resulting in a pulsating trend. A close inspection shows the peaks of pulses are higher during sleep in comparison to day time.
Insufficient sleep may disrupt this natural rhythm, causing in higher than optimal levels in the morning.
That's why night shift employees and those with abnormal circadian rhythm may observe unexpected results from their TSH blood tests.

TSH levels change throughout the day
"Circadian and 30 Minutes Variations in Serum TSH and Thyroid Hormones in Normal Subjects" by Weeke and Gundersen in Acta Endocrinol (Copenh), 1978, Vol. 89(4), pages 659‐672.
The pregnancy hormone, hCG, human choriogonadotropin, weakly stimulates the thyroid, as hCG has a structure similar to TSH.
Both of them drop together, especially in very early stage of pregnancy.
Therefore, trimester specific ranges of thyroid hormones should be used by labs to test pregnant women (Laurberg 2011).
Optimal TSH levels are very important for a baby's development and normal pregnancy.
The plot below shows mother’s hormone levels by week of pregnancy.
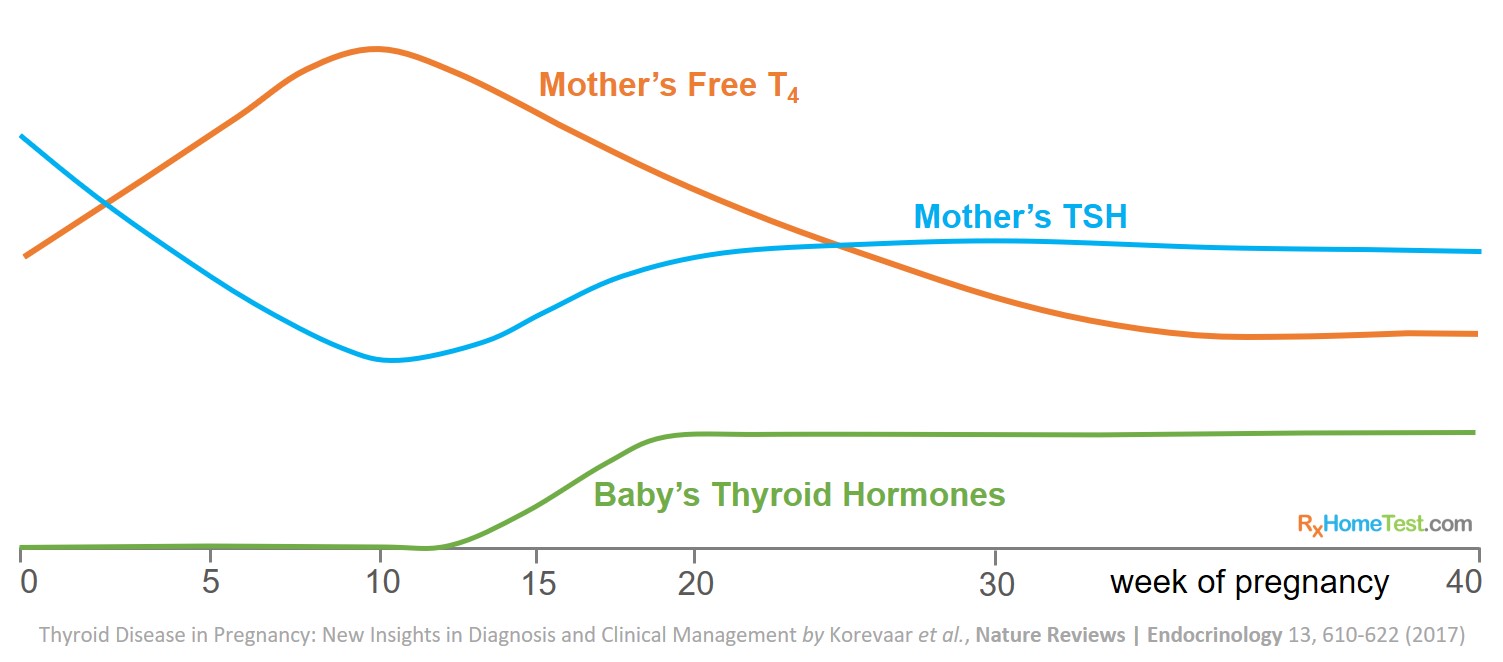
Chart showing TSH, T4 levels during pregnancy
"Thyroid disease in pregnancy: new insights in diagnosis and clinical management" by Korevaar and others in Nature Reviews Endocrinology, 2017, Vol. 13, pages 610–622.
Illness may affect functions of hypothalamus, pituitary and thyroid glands. This may result in low levels.
Medication for certain illnesses might affect the thyroid function.
During recovery from illness, levels might temporarily spike as thyroid stabilizes.
Obesity and overfeeding increases pituitary and thyroid function. This may result in higher levels (Laurberg 2011).
Always ask the lab for normal range of your test. This is the range you should monitor since values vary as part of the normal sample processing.
TSH rises with age. And the correlation is almost linear (Hollowell 2002).
The risk of thyroid problems among 80+ year old is almost 5-times those below 50. This holds despite gender, race, and geography affecting the gland.
In almost every age group, women tend to have higher values than men.
The risk of abnormal levels is highest in older women and lowest among most men.
Thyroid Stimulating Hormone levels continuously increase with age.

TSH levels chart with age
"National Health and Nutrition Examination Survey (NHANES III): Serum TSH, T4, and Thyroid Antibodies in the United States Population (1988 to 1994)" by Hollowell and others in The Journal of Clinical Endocrinology & Metabolism, Vol. 87(2) 1 February 2002, Pages 489–499.
High values are likely sign of an underactive thyroid gland. It is forcing the pituitary gland to release more hormone, a condition known as hypothyroidism.
Values over 10 mIU/L is overt or clinical hypothyroidism. Studies show it results in higher levels of cholesterol—both total and low-density cholesterol (Mason 1930).
Mildly elevated values (above 4.5 mIU/L) are a known risk factor for future overt hypothyroidism.
The slow increase in Thyroid Stimulating Hormone with age is unharmful and might, in fact, help in longer life despite some risk of cardiovascular disease (Atzmon 2009, Rozing 2010, Gussekloo 2004).
Low values are indication of hyperthyroidism. It is likely sign of an overactive thyroid gland that is producing high levels of thyroid hormones, T4 and T3 (Pantalone and Nasr 2010).
Abnormally low (less than 0.1 mIU/L) values are almost always an indication of overt (or clinical) hyperthyroidism (Helfand 2004).
Elevated T4 and T3 with abnormally low values may indicate nodular thyroid disease or an autoimmune Grave’s disease.
There is good evidence that undetectable low values (less than 0.1 mIU/L) increase the risk of atrial fibrillation later in life (Helfand 2004). These correlate with higher probability of stroke. In one study of those older than 60 years, the risk of atrial fibrillation over 10 years was around 32%. In comparison, the risk is 8% in people with healthy levels (Sawin 1994).
Some studies suggest low hormone results in loss of bone mineral density and bone fracture. However, this seems true only for vertebral fracture. Data do not suggest any correlation to hip fracture (Helfand 2004).
Low values (0.1 – 0.4 mIU/L) should always follow a measurement of T4 and T3, according to recommendations from theCleveland Clinic Journal of Medicine. They should be rechecked within few weeks to confirm the results and to avoid potential variation due to a one-off event.
Well known symptoms of high values include:
Intolerance to cold (compared to those around you)
Weight gain
Loss of appetite
Low energy and weakness
Coarse dry hair
Dry rough skin
Fatigue (which can happen with both low and high values)
Common symptoms of low levels include:
Intolerance to heat (compared to those around you)
Palpitations
Anxiety
Tremors
Difficulty in sleeping or insomnia
Unusually high appetite and weight loss
Fatigue (which can happen with both low and high TSH)
Samples from Framingham Heart Study show a linear correlation between gain in weight and high TSH values. The data suggest women show larger weight gain.
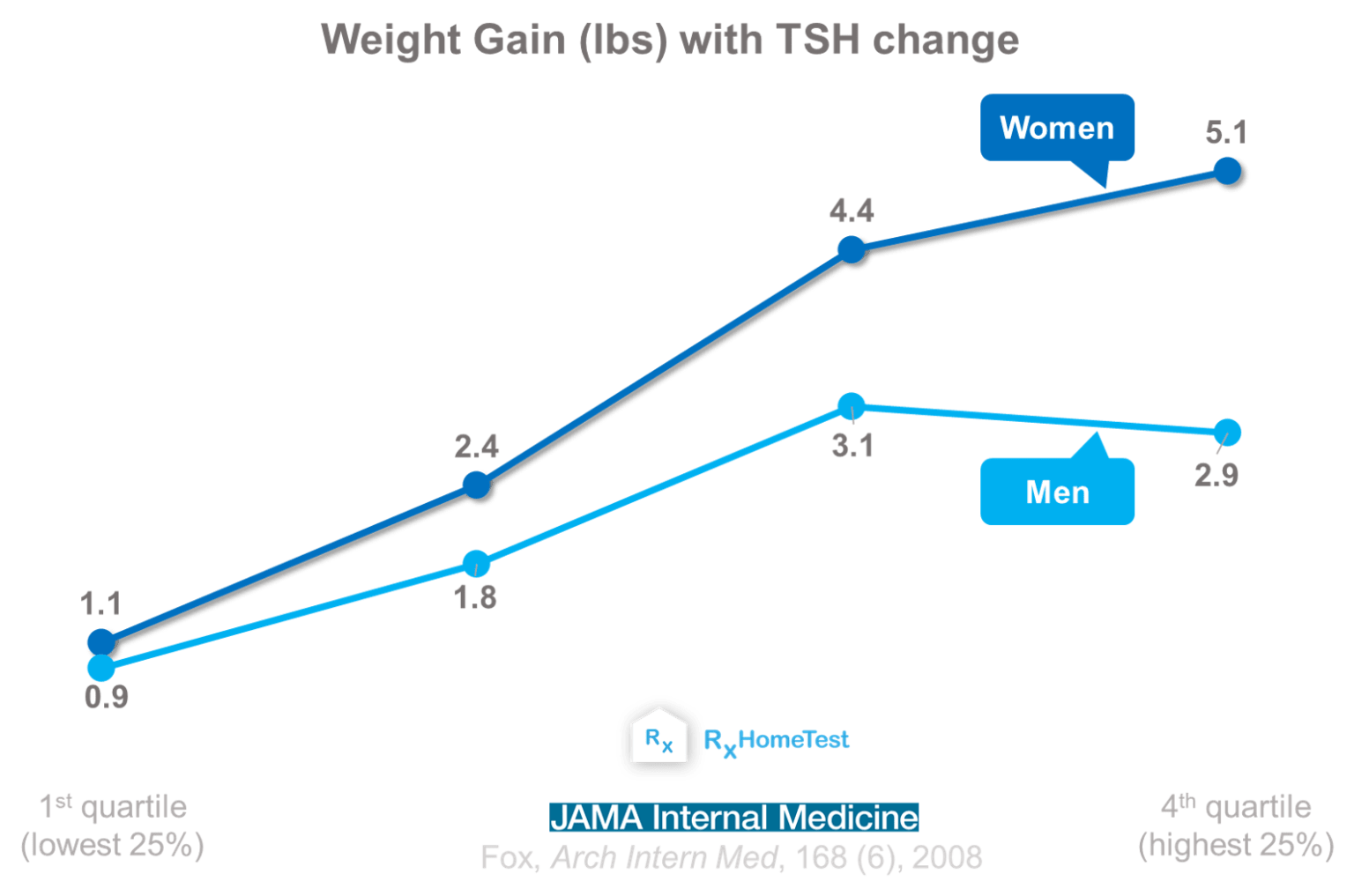
Studies show women tend to gain more weight with changes in TSH levels
"Correlation of Thyroid Function to Body Weight – Cross-sectional and Longitudinal Observations in a Community-Based Sample" by Caroline Fox and others in Archives of Internal Medicine, Vol 168 (6), MAR 24, 2008.
Another chart below shows an average weight gain after 6-months of testing. Weight increases almost linearly with higher values. Similar gains have been reported after 5 years, except for those with values above 3.6 mU/L. They gained over 10 lbs!

Chart showing more weight gain with higher TSH changes
"Small Differences in Thyroid Function May Be Important for Body Mass Index and the Occurrence of Obesity in the Population" by Nils Knudsen and others in The Journal of Clinical Endocrinology & Metabolism, Volume 90 (7), July 2005, Pages 4019–4024.
Thyroid health is determined by the hypothalamus-pituitary-thyroid (HPT) axis. One gland often tends to compensate for abnormal behavior of another to maintain a balanced cycle.
Whenever thyroid cannot release sufficient T4, the pituitary compensates by releasing more TSH (or vice versa). Therefore, knowing TSH alone might not be sufficient for a full diagnosis.
There is a well known linear correlation between age and Thyroid Stimulating Hormone. However, T4 values do not show any correlation with age. Therefore, with advancing age, there is a lower pituitary response to thyroid function which a TSH test alone might not capture.
If TSH values are abnormal, one should check T4 and T3 for thyroid dysfunction. Also, checking for TPO antibodies can help assess the presence of autoimmune thyroid disease (Glinoer and Spencer 2010).
Autoimmune diseases–and presence of TPO antibodies–in certain groups can be very high, e.g., elderly white women have a rate of almost 50% positivity (Laurberg 2011). Those aged 55+ years with TSH above 4.5 mIU/L have a rate of 36-76% (Boelaert 2013).
In some cases, e.g., during pregnancy, a combination of thyroid dysfunction and high TPO antibodies may predict complications in pregnancy and mother's risk of dying later in life (Männistö 2010).
If your levels are outside normal range, a repeat test is very useful. In one study, repeat of 400,000 patients after 5 years suggested that only 2% had developed abnormal levels. And 50% were within healthy levels (Meyerovitch 2007).
How do you know whether a high value was not a random event? Analytical studies suggest a deviation of 40% or higher, from last measurement, is not a random event (Karmisholt 2010).
Mean values of healthy Thyroid Stimulating Hormone in a person are mostly determined by their genetics. However, environmental factors can affect them considerably (e.g., iodine content in food).
One should carefully review the lab ranges in their TSH test results. Some experts suggest values up to 10 mIU/L might not require any medicine; levothyroxine prescription for such cases may not show any benefit (Ross, 2022).
The variation is much narrower for individual person in comparison to population variation. There is about 50% tighter variation in comparison to data for large population.
TSH is the most sensitive indicator of thyroid gland function when pituitary-hypothalamus function is healthy. For example, a thirty percent reduction in T4 results in a sixfold increase in TSH (Eisenberg 2009).
The TSH upper reference limit: where are we at? by P Lauerber et. al., Nature Reviews Endocrinology 7, p232-239 (2011).
Approach to a low TSH level: Patience is a virtue by K Pantalone and C Nasr, Cleveland Clinic Journal of Medicine, 77 (2010).
Serum TSH determinations in pregnancy: how, when and why? by D Glinoer and C Spencer, Nature Reviews Endocrinology 6, p526–529 (2010).
Circadian and 30 minutes variations in serum TSH and thyroid hormones in normal subjects by J Weeke and H Gundersen, European Journal of Endocrinology 89(3), p659-672 (1978).
Serum Thyrotropin Measurements in the Community by Meyerovitch et al., Arch Intern Med 167(14), p1533-1538 (2007).
Screening for Subclinical Thyroid Dysfunction in Nonpregnant Adults: A Summary of the Evidence for the US Preventive Services Task Force by M Helfand, Ann Intern Med 140, p28-141 (2004).
Treating hypothyroidism is not always easy: When to treat subclinical hypothyroidism, TSH goals in the elderly, and alternatives to levothyroxine monotherapy by DS Ross, J Int Med 291(2), p128-140 (2022).
